INTRODUCTION
The detection of anti-HLA antibodies helps to predict both the function and survival of transplant allografts.9 Most allograft damage is mediated though the activation of complement; C4d deposition is widely accepted as a marker for antibody-mediated rejection in renal allografts.1
DETECTION OF ANTI HLA ANTIBODIES
Laboratory testing before transplantation includes cross matching donor cells (lymphocytes as surrogates of renal cells) with recipient serum. If a recipient has antibodies against a donor’s HLA type, the antibodies will bind to the donor’s cells and the crossmatch should be positive, whereas if the recipient does not have anti-HLA donor-specific antibodies, the crossmatch should be negative.
The transplant based on both a negative complement-dependent cytotoxicity (CDC) and the more sensitive flow cytometric crossmatch. However, both can be subject to interference, 2,3 and even
if both crossmatches are negative, early graft rejections still occur. Higher organ rejection rates occur among patients with donor specific anti-HLA antibodies prior to transplantation.4
The presence of preformed human leucocyte antigen (HLA) donor specific antibodies (DSA) is a major risk factor for early renal allograft rejection and graft loss [5,6]. Different techniques are currently available to detect anti-DSA in sera from patients waiting for a graft.
- The standard complement-dependent cytotoxicity crossmatch (CDCXM) and some modification of this technique such as the anti-human globulin-augmented assay (AHG-CDCXM) have been the most widely used to detect anti-DSA before transplantation [7-9]. The widespread utilization of CDCXM against donor T lymphocytes has resulted in the almost complete elimination of hyperacute rejection [10-12].
- The flow cytometric crossmatch (FCXM) is more sensitive than CDCXM [10–12]; nevertheless, this technique is not specific because it can detect antibodies directed against cell surface antigens irrelevant in the outcome of the graft. The issue of FCXM being a more sensitive but less specific technique when compared with CDCXM, leads to false-positive results, preventing the opportunity of a transplant in patients without relevant DSA.
- The single-antigen bead flow Cytometry (SAFC) allows the determination of the presence of DSA comparing the HLA typing of the donor with the repertory of anti-HLA antibodies against recombinant HLA molecules in the serum of each patient (virtual XM)
SINGLE ANTIGEN BEAD TECHNOLOGY IS USED TO DETECT HLA ANTIBODIES
The Luminex anti-HLA antibody detection assay is reportedly more sensitive and specific than either the CDC or flow cytometric crossmatches.4,13,14 In fact, some consider the Luminex antibody detection technique to be the new gold standard for identifying anti-HLA antibodies.5 This technique is a solid-phase assay in which purified HLA molecules (either of a single HLA type or a combination of types) are attached to beads. These molecules will bind to anti-HLA antibodies in the patient’s serum.4,14 Using single antigen technology, the Luminex technology can predict a patient’s sensitization to particular HLA types prior to transplantation without performing a physical CDC or flow cytometric crossmatch (termed a ‘virtual crossmatch’).
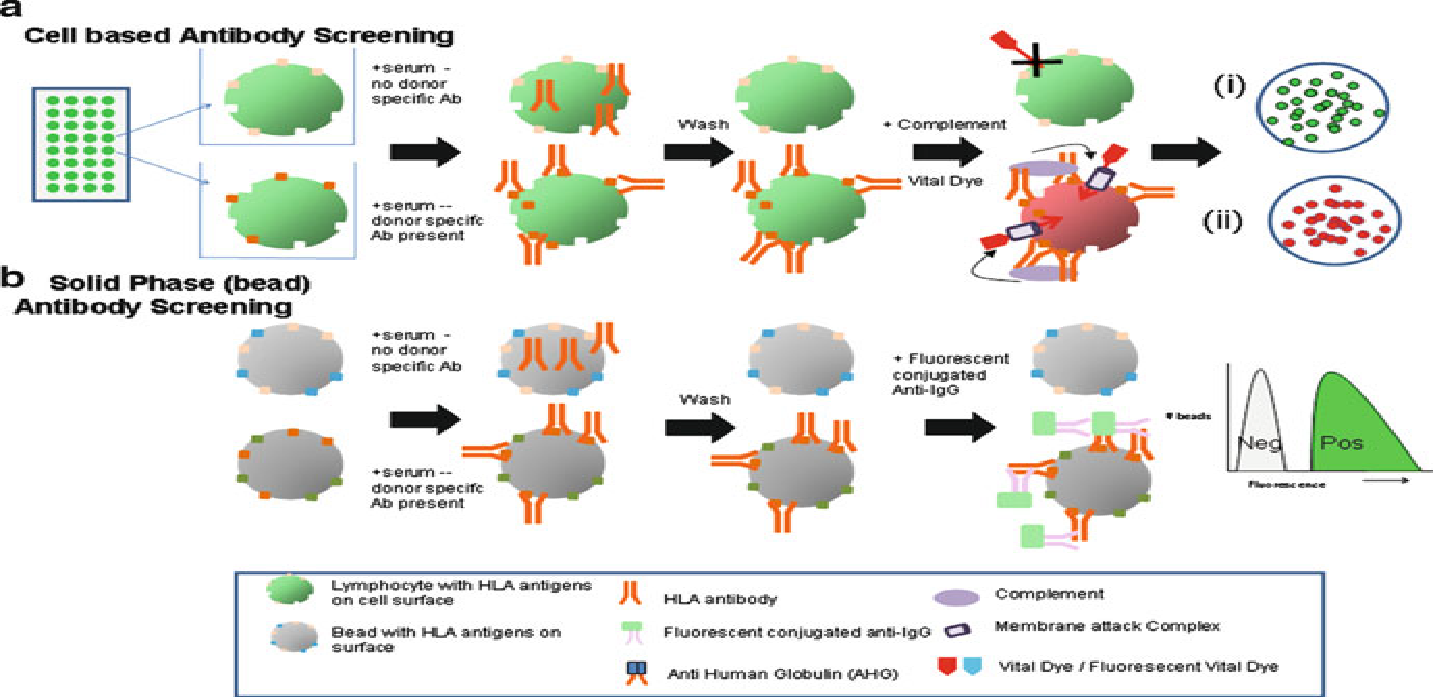
Schematic representation of Cell Based & bead based Antibody screening
Comparison between Antibody detection parameters of cytotoxic vs. bead based antibody screening tests
COMPARISON ANTIBODY DETECTION PARAMETERS OF CYTOTOXIC
PARAMETER
|
CYTOTOXIC ANTIBODY SCREENING
|
BEAD BASED ANTIBODY SCREENING
|
Detects class I HLA Ab
|
Yes
|
Yes
|
Detects class II HLA Ab
|
If B Cells are used
|
Yes
|
Detects non-HLA Ab
|
Yes – to any target
on lymphocyte
|
Only with antigen-specific
assays (e.g., MICA)
|
Detects low titer Ab
|
No
|
Yes
|
Able to identify HLA Ab
to specifi c antigens
|
Rarely
|
Yes (using single antigen
beads)
|
Detects noncomplement
binding Ab
|
No
|
Yes – all IgG subtypes
detected
|
UTILITY OF SAB TESTING
Donor specific anti HLA antibodies (DSA) as the term expresses are anti HLA antibodies directed against the donor cells. DSA may be detected by cell based methods such as microlymphocytoxicity and flowcytometry or by solid phase immunoassay (SPI) which includes Luminex and ELISA. As per guidelines of consensus conference held at Rome in May 2012 a patient must be tested by both cell based methods and SPI15. The IgG isotype anti HLA donor specific antibodies are most relevant in graft rejection. One method which is widely used in USA and EU is single antigen bead testing (SAB). Advantages include no requirement of donor cells unlike the present DSA and hence no viability issues and availability of clear cut guidelines for risk stratification of patients. Some aspects of SAB testing are brought out in this issue.
SAB testing may be done if PRA screen is positive and detects anti HLA class I (ABC) and anti HLA class II (DR, DQB1, DQA1 , DPA1, DPB1, DRB3, DRB4 and DRB5 antibodies. This implies that if anti donor antibodies are identified, the donor may require (high HR) resolution typing if the antigens in the donor at low resolution are same as the alleles against which the antibodies have been detected. e.g. If anti A*02:27 antibodies are present in recipient serum and the donor’s HLA A antigens are 03, 24 no HR typing of donor shall be needed which would have been required if the donor is HLA –A 02, 30 as he could be having any of the more common HLA A 02 alleles. Additional HR HLA typing may be required for the respective loci if recipient serum has anti DPB1, anti DPA1, anti DQA1 and anti DQB1 antibodies. Normally in India the immunological work up does not include typing at these loci. This will mean increased cost for the patient. DSA detected by CDC crossmatch are a contraindication to transplant whereas antibodies detected by other methods imply enhanced risk.
DSA have a role in both acute and chronic antibody mediated rejection (ABMR), for which it is a good non invasive test and is superior to Luminex crossmatch which does not detect anti HLA C, anti DPB1, anti DPA1 anti DQA1 antibodies. The positive predictive value of DSA on histological changes is not great, but the negative predictive value generally excellent. To state it in another way, the presence of DSA does not accurately predict ABMR in allograft biopsy, but the absence is suggestive of lack of antibody mediated injury16.
Otten et al. recently described that only if both class I and II antibodies are present simultaneously, they may be associated with increased risk of graft failure16. These “double positive” patients have an increased risk of graft failure as compared to patients with only HLA – class I or only HLA –class II antibodies.
British Transplantation Society and British Society of Histocompatibility Guidelines for DSA18
Intestinal and multi-visceral transplantation: Table 1 shows the level of risk along with MFI
Risk Level
|
MFI
|
Description
|
I
|
No detectable
Antibody
|
Standard
|
II
|
<2000
|
Minimum risk of hyperacute rejection due to low level of HLA DSA but greater than standard risk of rejection
|
III
|
2000 -8000
|
Flow cytometric crossmatch likely to be positive, conferring an intermediate risk of ABMR
|
IV
|
>8000
|
CDC crossmatch likely to be positive conferring a high risk of ABMR
|
Frequency of testing: At three monthly intervals; also antibody screening and specificity testing should be done on two separate samples at different time points.
HLA class II antibodies pose a significantly higher risk for both kidney and liver transplant recipients.
Post-transplant DSA monitoring in recipients with preformed DSA
Luminex is able to identify preformed DSA in more recipients. Transplants in patients with DSA identified by CDC crossmatch should be avoided. A positive flow crossmatch and DSA detected by SAB indicate higher risk of acute and chronic ABMR and patients may require desensitization. Post-transplant anamnestic response can lead to rise in DSA titers. Unsensitized recipients may also show presence of DSA associated with graft dysfunction.
Frequency of post transplant DSA test: University of Michigan recommendations
- High risk – includes those with PRA >20%, Retransplant s, those with African ethnicity and history of acute cellular rejections: at 3, 6 and 12 months post-transplant.
- De novo DSA may be transient and if low titer requires monitoring; high titer DSA or DSA in setting of stable renal function requires allograft biopsy. If the biopsy is normal, management of DSA is not clear.
No comments:
Post a Comment